

Laparoscopy Laparoscopic Exploration
Introduction
When it is difficult to make a definite diagnosis through laboratory examination and a variety of imaging diagnostic techniques, laparoscopy shows its unique and important role in accurate diagnosis, which can make up for the shortcomings of laboratory examination and imaging examination.
Laparoscopic exploration has less complications and less pain. It can not only directly observe the normal organs and pathological tissues, but also biopsy under direct vision, obtain the evidence of disease examination, accurately evaluate by surgeons, and assist in treatment. For the latter, surgical treatment is feasible immediately.
On a quite large scale, laparoscopic exploration replaced the previous exploratory laparotomy and avoided blind laparotomy as much as possible. In terms of diagnosis, it is applied to the diagnosis of abdominal trauma, hepatitis, tuberculosis, ascites, abdominal mass, abdominal metastatic cancer and liver cancer. For tumor staging and preoperative staging of intra-abdominal malignant tumors, laparoscopy is accurate, which can avoid unnecessary open exploration.

Laparoscopic surgery is what we often call “perforation” surgery. In fact, laparoscopy is not only used for surgery. Laparoscopy has the following three characteristics in the field of surgery: it can be used for diagnosis and treatment, as well as minimally invasive surgery.
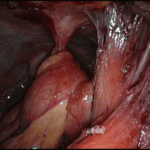
Laparoscopy is almost everywhere. More than 95% of the abdominal and pelvic organ operations can be completed under laparoscopy. Laparoscopy extends the surgeon’s line of sight into the abdominal cavity without opening the abdominal cavity. Laparoscopy can clearly enlarge various organs in the abdominal cavity, and various lesions on its surface can be clearly seen. The images seen can be saved by computer.
Why Laparoscopic Exploration
Laparoscopic exploration can make up for the shortcomings of traditional imaging examination and provide a reliable basis for further clinical diagnosis. In the diagnosis of many difficult and miscellaneous diseases in abdominal surgery, such as unknown acute and chronic abdominal pain, the accuracy of laparoscopic diagnosis is much higher than that of B-ultrasound and CT, so as to avoid the delay of the disease caused by unknown diagnosis.
Not only that, once diagnostic laparoscopy is clearly diagnosed, most diseases can be cured directly under laparoscopy. More importantly, it is a minimally invasive operation, which only causes minor trauma to patients.
General Laparoscopic Diagnosis
Indications
- Diagnosis of unexplained acute and chronic abdominal pain
- Exploration of abdominal injury
- Staging of abdominal malignant tumors
- Biopsy and differential diagnosis of liver diseases
- Differential diagnosis of ascites
- Diagnosis of gynecological infertility
Contraindication
- Severe cardiopulmonary dysfunction
- Hemodynamic instability
- Uncorrectable coagulation dysfunction
- Severe liver dysfunction or massive ascites
- Severe abdominal wall and intra-abdominal infection
- Multiple abdominal operations are estimated to have extensive abdominal adhesions
- Large hiatal hernia
- Diaphragmatic rupture
- Mechanical or paralytic ileus
Laparoscopic Diagnosis Of Non Traumatic Acute Abdomen
Indications
- Unexplained acute abdomen
- Acute nonspecific abdominal pain (NSAP)
- Those who have been diagnosed with symptoms and are not satisfied with the boost and need further diagnosis
Laparoscopic Diagnosis Of Abdominal Injury
Indications
- Minor open wound of abdominal wound
- Patients with simple closed abdominal trauma suspected to have substantial organ rupture but no obvious hemorrhagic shock
- Patients with simple closed abdominal trauma have signs of peritonitis, their vital signs are still stable, and they are suspected to have rupture of hollow organs
- The change of the condition cannot be explained by the injury of other parts, and it is suspected that there is abdominal organ injury
- If there are multiple combined injuries, it is necessary to run out of the abdominal organ injury and deal with other injuries again
Contraindication
- Patients with severe hemorrhagic shock, unstable vital signs or severe peritonitis after abdominal trauma decide to perform exploratory laparotomy
- Open abdominal trauma with large abdominal wall defect
- Severe chest and brain injuries
Advantage
- The diagnosis can be made as quickly as possible to reduce the negative exploratory laparotomy rate
- It can achieve the integration of diagnosis and treatment, and reduce the rate of therapeutic laparotomy
- Know the choice of incision and operation method of laparotomy
Downside
- It is not applicable to all patients with abdominal trauma. For signs of hemodynamic instability or severe peritonitis, exploratory laparotomy must be performed
- In addition to the common complications of laparoscopy, there is a risk of tension pneumothorax in patients suspected of diaphragm injury
- For retroperitoneal injury, only indirect evidence is provided, such as retroperitoneal hematoma, pneumatosis, bile staining, etc., but the injured organs and parts (such as duodenal injury, ureteral injury, kidney injury, etc.) cannot be accurately provided
Common Issues And Countermeasures of Laparoscopic Exploration

(1) Master the indications. Abdominal pain occurs repeatedly for more than half a year. The effect of conservative treatment is not obvious. Multiple examinations can not be confirmed. Abdominal signs are relatively light when abdominal pain occurs, and the site of abdominal pain is relatively fixed. There is a history of surgery in the past;
(2) Laparoscopy has a certain negative exploration rate, so it is necessary to communicate with patients and their families in detail before examination;
(3) Laparoscopy is helpful to observe the surface of viscera, but it is difficult to observe the interior of solid viscera, retroperitoneum, mucosa, bile duct and urinary tract lumen. Therefore, corresponding examinations must be done before operation to eliminate them;
(4) Don’t be satisfied with finding a lesion during exploration, but conduct a comprehensive exploration of the abdominal cavity to prevent the omission of other lesion sites;
(5) Female patients are referred to gynecologists for intraoperative consultation.
Precautions for laparoscopic exploration
#1. Hematocele
After absorbing the accumulated blood and washing the abdominal cavity, look for the bleeding spot.
Ectopic Pregnancy
- Bleeding characteristics: more pelvic hematocele.
- Treatment: salpingectomy may be considered
- The difference between pelvic cavity and abdominal cavity
Liver And Spleen Injury
Characteristics: more blood accumulated in abdominal cavity
Treatment:
- liver subcapsular hemorrhage and mild liver parenchymal rupture hemorrhage: laparoscopic repair
- Severe liver parenchyma rupture and bleeding, or bile leakage: conversion to open surgery
- Splenic rupture and hemorrhage: preserving or cutting the spleen according to the degree of rupture.
#2. Inflammatory Exudates, Perforated Ulcers (Gastrointestinal Contents)
- Searching for the primary lesion after peritoneal lavage.
- Common primary lesion: perforation of gastroduodenal ulcer, acute appendicitis, acute cholecystitis, acute pelvic inflammation
- Treatment:
corresponding treatment, details omitted.
#3. Adhesion
- Check the history of previous operation and peritonitis. [why is there intestinal adhesion after operation?]
- Treatment: adhesion lysis.
#4. Tubercle
- Nodules can be seen in the liver, peritoneum and pelvic cavity
- Treatment: combined with laparoscopic ultrasound for diagnosis and staging, the patients were treated accordingly.
Thanks for reading, we hope you have enjoyed the content.
If you are looking for the endoscopy equipment, feel free to check our product page or contact us at our contact page.





Leave a Reply
Want to join the discussion?Feel free to contribute!